
The weekly “little of this, little of that” feature here at Like Mother, Like Daughter!
Despite our current state of discombobulation (and we will update you soon! We keep saying that! But we do try! It just keeps happening! We're hanging over here, no energy left for blogging!), we have a giveaway for you for First Communions (and really any event that begs for a solid beautiful gift).
Sacred Art Series is offering to two Like Mother, Like Daughter readers the beautiful Gospel of St. Luke and St. John. 
What can I say about this volume? It's just perfect for devotional reading. See how it doesn't have verse numbering and footnotes (although it does have headings and references)? Of course there's a place for those, in your regular study Bible. But for praying with Scripture, The Gospel of St. Luke and St. John fits the bill. (Can we convince them to publish a companion Gospel of St. Matthew and St. Mark?!?)
The type is a bit larger, so children can follow along easily. And of course, the artwork is fabulous. Throughout the pages are beautiful masterworks that radiate the goodness of God's Holy Word. The artwork adds more scope for meditation.
This is an Amazon giveaway — just enter using this link. (I don't receive anything for this giveaway — I'm just a great fan of this particular volume!)
Will Bloomfield, the publisher of the Sacred Art Series, is also offering a daily reading from St. Philip Neri in your inbox.
And for two weeks, the Gospels will be reduced 25% — from $39.95 to $29.95. So do take advantage if you aren't a winner of the giveaway!
On to our links!
- Can hospital buildings — and health care — be oriented to the beautiful? David Clayton recounts a lecture by a Catholic doctor on the subject, adding his thoughts and some revealing photos. I would add that it's worth reading God's Hotel, a book by a doctor who is not Catholic, that offers the perspective of someone who worked in the last of the medieval-based almshouses in the US (in San Francisco!) before it was “renovated” for modern efficiency by experts. (I got it out of the library.)
- Of course we are still celebrating Easter! A really good meditation on the question of truth.
- Speaking of videos, and if you come to a day when everyone is sick and needs to sack out in front of soothing ones, here are some: craftsmen making a dugout canoe, and a knife, and a longbow. Our dear friend Jana says: All the other videos on the “northmen” vimeo site that I've seen are great to show the kiddos. (These are the kind of videos that we watch to supply for the lack of tradesmen in this world. The children will watch men working for hours in complete silence!)
- This review reveals a lot about the current state of what passes for education in our society: Pedagogy of the Distracted.
- My husband's take on Rod Dreher's Benedict Option: It doesn't go far enough. Interestingly (and a bit of a surprise to me), we are in Rod's book Crunch Cons — he says that we “settled around a monastery” — but that's not exactly true, as Phil explains here.
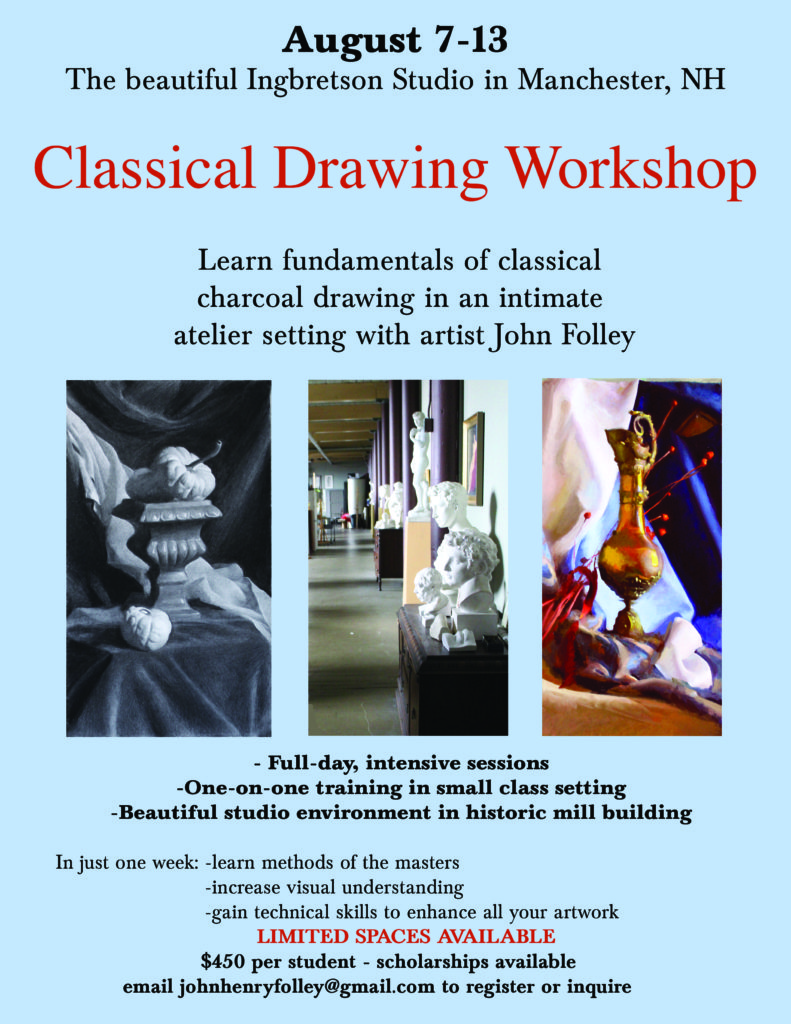
- A wonderful opportunity — a classical drawing workshop in a fabulous setting! I happen to have a direct line to the experienced artist-teacher (he's literally standing in front of me), and he says it would be excellent for anyone aged 10 to 100 — anyone at all who is interested in gaining more expertise in artwork:
I hope you are enjoying — truly enjoying and basking in! — the Octave of the Glorious Resurrection of Our Lord!
From the archives:
- Are you (or is one you love) gearing up for wedding planning? Do dip into our wedding posts!
- As the seasons change, it's always good to revisit menu planning, the key to sanity!
~We’d like to be clear that, when we direct you to a site via one of our links, we’re not necessarily endorsing the whole site, but rather just referring you to the individual post in question (unless we state otherwise).~

I can’t begin to tell you how happy I am to read the article about the physical environment of hospitals and medical facilities. I’ve long railed (to myself, natch, while driving around) against the truly depressing look of the nursing home and extended care facilities in my neck of the woods. We’ve begun checking out assisted living places for my MIL, and let me tell you…unless you’re made of big $$$, you’ll live out your last days in what amounts to a barracks. A recent tour of the affordable assisted living/extended care place here left me in tears (which began with the striped mauve and pine green ’80’s wallpaper and went downhill from there). The little touches of humanity were superficial at best.
Catholics own the idea of dignified health care. It’s our legacy! The Carmelites of the Aged and Infirm’s foundress, Mother Angeline McGrory, now a canonized saint, pioneered treating the whole person in a homelike atmosphere, and established a new branch of the order expressly for this purpose. In my mind, I see nursing home design incorporating elements of a cloisters, with rooms that open out on their little garden, or a shared park. (I remember realizing this when watching the movie “Into Great Silence”, and thinking, wow…I could die happy in a place like that, no prob.)
This would require more than money – it’s really a sea-change in our regard for the elderly.
Yes! My husband’s grandmother died last year … before that she was the type of woman who scrubbed her own windows and baseboards, cooked her blintzes from scratch, walked everywhere. But she went into the hospital after some heart troubles, they gave her an antibiotic that caused a severe immune reaction, she wound up in the I.C.U. The experience — the constant beeping, the eerie light at every hour of day and night, the lumpy bed from which you are not allowed to leave, even to use the toilet, the finger pressure cuff, the hundreds of anonymous people coming into her room but not talking to her every day, the severely regulated, unappetizing food — really caused huge physical and cognitive declines. She eventually got out of the hospital and then into a (slightly less dire) rehab facility for weeks and then back to her daughter’s house, but she never returned to her apartment and when she had another spell, they took her to the hospital again. Two trips to the hospital were enough to do her in. It is still shocking to me how quickly she declined after each hospital stay. We really need to think about what makes humans feel happy and healthy in Homelife and try to make that, as much as possible, accessible to people when they are ill. Hospitals are really just treating humans as meat machines with various input and output metrics that must be managed to a certain range. All the people in them are very caring and do their best, but the environment is so inhumane.
I loved the book God’s Hotel because it really did seem to get at the idea that we humans are truly whole people, both body and soul, and that both need to be nourished, given solitude, companionship, rest and stimulation in order for us to heal.
Auntie Leila,
Thank you for posting the video on making English longbows. A few years ago, my (now 17 year old) son began making longbows. They are beautiful works of art, and we’ve been trying to encourage him to sell them. Some of the woods that he has used are exotic species – most I’ve not heard of before: purple heart, padauk, wenge… He stopped making bows because he developed a passion for go-karts, having built 2 of them from the ground up now.
This video came at a good time, because my son recently announced that he’d like to start making bows again. I think it was good inspiration for him (and his younger brothers – who all like to accompany my husband to the archery range together- watched the video too). Please offer up a prayer that if this is what God wants Caleb to do, he’ll respond to that call. He’s our oldest child (we’ve 8 in all) and navigating how to guide them in life (especially the pre/early adult years) is new to us. Thank you!!
In Christ,
Melisa
Wow, Melisa, that is amazing! We will pray for him!
The Pontifex University post was interesting (although with an surprisingly high level of typos), but I would note that not all modern hospitals are lacking in beauty (some have lovely atria and have pleasing architectural lines, if not of glorious old stonework) and that some modern innovations (like the most recently built hospital I’ve seen, with individual rather than shared rooms – the glories of being able to rest except when nurses are checking on/tending to you specifically! of having your own window and space where you do not need to worry about disturbing anyone else!) are a wonderful thing for patient care.
I do think beautiful communal spaces are excellent for reasonably-well-functioning convalescents, generally, but hospitals increasingly send people home to convalesce, rather than wheeling them around public areas, and for the very sick, a reduction in disruption and chaos (while still having the benefits of natural light, etc.) is an incredibly helpful thing for healing. If the only exposure you have to the beautiful architecture and courtyards and facades is *perhaps* once upon entrance and exit, and via proxy as nurses/doctors walk through them, that is still potentially of some benefit as the uplift to medical staff transfers to care. However, the interior rooms and the way they’re laid out are of more immediate import to actual patients, and many old buildings fall short in the beauty (and function) of the spaces not intended for large gatherings. In short, the way a building functions and feels for a visitor, with the areas one is most exposed to as a visitor (the hallways! the walkways! the courtyards! the entrances! so photogenic!), is different from the way a building functions for a bed-ridden inmate who *might* get wheeled through the sweeping arches once or twice during the course of their entire stay (but might not even be conscious for those portions). I’d vastly rather have windows I can see the sky from, plants, and privacy during all my waking hours, than get to see a heaven-lifting arch for five minutes, twice, bookending the however-many-day stay, and otherwise have no view of the world outside (and no option for plants inside) for the entirety of my time “in residence.”
Where one can have both, that is excellent, as when one can combine beauty and functionality in a household object. But many old buildings *don’t* do both – they’re not functionally wheelchair-accessible, not built on the outside to be divided into many rooms on the inside (I presume you don’t particularly want a return to the large open wards of 12+ beds each?) while still giving each room natural light, and simply not structured to provide easy access between necessary points (ah, stone-cold hospital food because of sheer distance). Of course, one can also end up with the option of “neither” – buildings that are ugly on the outside and inside, and also lack function and light – but if one had to choose, I prefer modern buildings that take the patient, or inpatient, view substantially into account. (while still providing good hallways and a light-filled atrium for doctors/nurses/visitors)
There is also the question, of course, of the expense, but that’s a question for another time.
KC, you make some interesting points but I think you might find the book “God’s Hotel” making a different case.
I enjoyed the book! Thank you for the recommendation! I still think exterior architecture (in the afterword of the linked post) is vastly less important to patient health than the spaces that the patients are in, though.
And certainly, for long-term care of people who can cope with companionship/stimulation (which, as I noted, hospitals generally don’t do anymore), open wards or community spaces in the daytime would be great, provided 1. good supervision (which the book notes is the first thing to go with budget cuts), and 2. the option to move people who are having a harder time or being especially disruptive into a private space (a practice in the book, although probably not in medieval hospitals). I still think sleep is probably better in solitude, but for some categories of lonely patients, the daytime payoff of companionship might compensate for that.
But given 1. what hospitals now do and 2. the various institutional, budgetary, and personal forces moving against caring and attentive nursing, I think individual rooms beat out open wards by a long shot… and the two-bed curtain-divided room in many hospitals (but not the newest one I’ve been in) provides a sample of the worst of both worlds.
I would expect external architecture to be a factor in the “culture” of a place, but a pretty minimal one given the other pressures involved in modern medicine.
But yes, certainly, as God’s Hotel exemplifies, as long as we’re using proxy variables to measure health success, we’ll probably end up shoving medical practitioners (and the people hiring and scheduling them) towards frankly bad outcomes for both patients and economic efficiency. It’s probably worse there than in education, actually; getting lab tests done but then not really *looking* at the results, the 15-minute appointment length that doesn’t give time for communication or really thinking, trying medications but then not ever trying the removal of medications, the avoidance of “high-maintenance” patients (many of whom couldn’t even get health insurance until 2010), etc.
The “patient satisfaction” or “patient as a client” model is a slight improvement on the “patient as interchangeable gizmo with numbers” metrics model that seemed to precede it, but patient satisfaction is not identical with health, either, and while it leads to less beeping at night (hooray!) and slightly more listening to patients, it reminds me sometimes of the faux-interest forced by Joann’s Fabrics (for a while, anyway; I took a survey from them that asked if their clerks had said the required things), making the cutting-counter clerks ask what each person was going to do with their fabric – now, being asked what you’re making is *great* if the person actually is interested, but forced, scripted, resented interactions aren’t good for anyone. And while it’s nice that medical professionals ask about your holidays or whatever, I don’t want that to be required of them and especially do not want Forced Scheduled Chitchat to usurp time that would be better apportioned to examination and diagnosis and treatment. So many things wrong with the way stuff is run! Sigh.
I added it to my library list when I read the post! 🙂
But seriously, the focus in many modern hospitals on the medicine and testing while ignoring the patient’s immediate environment in terms of decent food, positive human contact, nature/beauty, and rest (all kinds of rest!) is a disservice to health – but one that I do not think would be at all repaired by a focus on large-scale architectural beauty. How is someone’s body supposed to heal when the environment they’re in won’t allow them to sleep for more than two hours at a time? (I’ll grant that a lot of mothers with newborns somehow survive this, but still! Sleep is important for function and healing!) And how is anyone supposed to remain cheerful trapped in one room under constant fluorescent lighting with the noise of one’s hospital roommate’s TV continually bickering in the background all day long? And plenty of old books attest to the discomforts, indignities, contagion, depression, and sleeplessness of large wards (while also noting the occasional positive human contacts made possible).
The best “healing situation” I think I’ve toured tended to only put one patient to a room but also had the option for all patients who can move (or be moved) to gather in a sort of community room, roofed with windows, with puzzles and books and plants (and possibly fish?) and the opportunity for conversation (which then allows those who are tired to withdraw back to their shell when they need rest). That had lots of light and air, lots of windows, no majestic architecture but pleasing interiors (for the most part; one hallway carpet was an outrage on color), and nowhere to trip. The second-best had private rooms each with a bathroom (immediate reduction in the number of people who see your hospital gown gaps right there!), one wall of windows, and multi-level lighting options including the option for a sort of glowy light behind the bed – enough to knit by or talk with people by at night, not enough to keep you awake – but no “community” option that I know of. But the rooms were incredibly restful and well-constructed.
What I’ve read about children’s hospitals seems to indicate that more of them are put together with the idea of keeping the patients calm and rested and cheered (and also adequately socialized) in mind.
I’ll be interested to read God’s Hotel and see what solutions are propounded. 🙂
I think some of your assumptions will be challenged by the book, which focuses on the medieval model for hospitals. The outside architecture is actually a small part of the equation. There is much more to it, and you might be surprised to find that privacy is not a priority — and you may find yourself agreeing, at least in the context of an almshouse. I’ve spent lots of time in many different hospitals, and the universal take-away is that no sleep is to be had. In fact, a friend who was recently there and who complained to the nurse about the ridiculous noise at night was told, “Oh, everyone knows you can’t get any sleep in a hospital!”
Certainly I have spent time in Boston Children’s Hospital, and I can tell you unequivocally that I find their idea of “cheerful” and “calm” quite the opposite! It’s very sad, because of course the people who work there are trying their best, but the ignorance of what David Clayton is talking about in his post regarding the unity of body and soul, and how that is expressed in the environment, is quite complete.
I agree mostly but I do think the need for privacy, may be a bit different in Laguna Honda — which as the author of God’s Hotel noted, was a place of last resort for the people who weren’t really expected to get better, per se. The people who were on the wards a long, long time, who had little-to-no family to visit them, and yet companionship would likely be a balm for them.
However, I do think private rooms are invaluable for people who are seriously ill but likely to be sick for a few days or a week and who are going to be inundated with visitors. When our 2-year-old was staying in the hospital, it was so important to have that private room, precisely so he could have companionship and round-the-clock presence of me and his dad and brother. The privacy is what facilitated the companionship he needed to maintain normalcy and connection.
The worst model is the one in the modern hospital, where you have a neighbor in the same room who is discussing or facing extremely dire personal life crises, separated by a mere curtain, but who you are supposed to pretend does not exist. There is no closeness and each patient is expected to shoulder their suffering on their own, yet in the presence of a person who they may not even speak to once.
Very true about the terrible, terrible curtain.
The distinction of the long-term (and indigent) patient is accurate, I think, and I was trying to indicate simply that I think it’s not actually a given that absolute privacy is what everyone needs — yet some obviously do.
And everyone needs quiet and rest — but I defy anyone to produce either in the modern hospital, where the trash is emptied at 4:45 am and the night nurse has to bang her computer cart (because she has to have a computer) into the bed…
The Laguna Honda model is completely unknown to us (I mean we can hardly even imagine it!) because the head nurse had her eye on *all* the patients at all times, and could determine who needed more privacy — whereas now, the nurses are at a station and have their eye on precisely no one.
Interestingly (re: mobility), Dr. Sweet makes the point that in the “new efficient” hospital, there is no place for the wheelchairs! So actually the patients are stuck until someone could fetch one from who knew where…
Totally agree about the sleep and rest. Spent a few nights in a hospital recently when my dad was ill and was surprised by how ill I felt from all the beeping, the eerie, light, the random people coming in for “checks” at 1am, 4am and 7am, etc. etc. etc. And those beds. And the having to call someone for something like going to bathroom. They are the most unrestful places. As if designed for that purpose.
I was actually able to approximately sleep through most of the nights in the private room! Most nights the nurses were amenable to evening requests to set up the IV so that it wouldn’t alarm overnight (either swapping the bag if it was almost out or turning the flow lower), so no nocturnal beeping or nurse interruption at all on those nights! I could have done without the 6am blood pressure check, but still: mostly quiet, I could keep the room TV off, about 4 out of 5 of the people coming in took their cues from the silence of the room and how tired I looked and tended to go about doing their thing quietly (the 1 in 5 “Let’s Cheer You UP!!!” dramatic entrances were… not helpful for my recovery at that time). In itself it was a fairly relaxing experience (with a few exceptions), and compared to the two-person room (with that curtain another commenter mentions, where you are supposed to pretend the other person doesn’t exist, which is horrible in all sorts of ways; plus two peoples’ worth of alarms going off all night long, etc.), it was sheer bliss.
Obviously someone with more social needs and less need for rest would profit less from the arrangement; I agree that the ideal setup would be very different in a non-acute situation, with convalescents or, yes, longer-term invalids who are not in acute please-no-stimulation phases of illness, although honestly I still think that a soothing/quiet (and therefore probably private) space to sleep in (whether that’s at night or not) would be valuable to almost anyone. But, I’ll get my hands on the book soon and see what I think from there. 🙂
The best “healing situation” I think I’ve toured tended to only put one patient to a room but also had the option for all patients who can move (or be moved) to gather in a sort of community room, roofed with windows, with puzzles and books and plants (and possibly fish?) and the opportunity for conversation (which then allows those who are tired to withdraw back to their shell when they need rest).
I work in a small, Catholic, community hospital that does a beautiful job of end of live care in a not so beautiful, very old building. It was recently bought out by a bigger, secular company who already reduced our palliative care team.
We have single rooms only which is ideal, but no community rooms. Unfortunately, if a patient is well enough to make it down to another room, they are out the door. Hospitals now are just a place to put an end to a crisis. Healing typically takes place in a skilled nursing facility, rehab facility, or home with services.
Off to add God’s Hotel to my reading list.
Mr. Lawler’s take on the Benedict Option is such a breath of fresh air. So lucid. I have been wanting the full Lawler perspective on it since the first time I heard of it. I also received that post as a great encouragement today, because I have been suffering greatly over my (beautiful, exceptional, but troubled) parish lately, and I am constantly tempted to the bitter feeling that my efforts are a waste. I felt braced after reading his words. I will not give up, not yet. God bless you, dear Leila and Phil, you shine a light on the way forward for us frightened young parents.
Thanks, Elizabeth! Your sweet words mean a lot! We are trying… and good work not giving up. Stay close to Jesus on the cross, no matter what…
I agree with Elizabeth W! Your husband’s article felt like a bit of a challenge in the same way this particular blog challenges me to truth and beauty. I just finished Esolen’s “Out of the Ashes” and I am eager to read “The Benedict Option” myself, glad to have your husband’s perspective.
Also…the article about the Substitute book…yikes. I always hear the phrase lately “the devil is in the distraction” and I my heart aches for this description of the classroom. I wonder what Anne Shirley would think!?! What she would do?!? And yet they mention how the children could focus during a story, during a narrative. Oh I loved this! Good books can save us and save our children…and our Good Shepherd knew this with His way of speaking to us!
Happy Divine Mercy Sunday!
Lent and Easter have had me thinking about bibles, specifically children’s bibles. Do you recommend them? If so, do you have a favorite? I found myself thinking one might be nice for my three year old this year but I never liked the one my family had when I was growing up, so I thought I’d get your opinion. 🙂 Thank you!
My whole family just sat in rapt attention at watching the canoe being dug out. Thank you for sharing!
I live in one of the communities profiled in Dreher’s book, and I think he gets a bit of a bum rap. Perhaps it was unfortunate that he chose the expression “Benedict Option” in the first place, because it gives people the false impression that he is advocating a monastic retreat from the world. A New Yorker profile actually claims that he thinks people should take vows!
In fact, this “new and very different” (to quote MacIntyre) Benedict option is fully engaged in the world. It is like Benedict of Nursia in that it recognizes that the state cannot be a support for the Christian life, and so it withdraws from political action as the primary means of advancing the Kingdom of God on earth. Unlike the early monks, though, we don’t live apart from from the world; we help each other grow in faith and love in the context of family life, jobs, parish involvement, neighbourhood activities, works of mercy, etc.
Hence, in practice, the distinction between reviving the Church and reviving the broader culture is not always as clear as Phil seems to suggest. For instance, our parish school’s curriculum is intended to form the minds and hearts of the parish’s children, but also of children beyond the parish, including non-Catholics; it is both a tool for vivifying the Church and a tool for evangelization. When we organize meals for a new mother, we’re helping her, and we’re also modeling community life to our neighbours.
Thanks for the recommendation! I’ve added God’s Hotel to my reading list. I have very strong opinions on hospital layouts! A few years ago, I had the opportunity to visit a hospice house in Peru. It was setup as a quad. All of the rooms were private but each opened into the garden. In the center of the garden was a small chapel with large glass-less windows. Those who were mobile enough could visit the chapel (wheelchair accessible of course) and the bed-bound could see into it from their rooms. There was a communal dining room for those able to get out of bed. The same meal was provided for all. The hearty chicken soup, made by the nurse that day, was puréed into different consistencies, depending on the needs of the residents. The hospice backed up on to a school yard, so the cheerful sounds of children playing were heard throughout the day. I was so impressed by the setup and as a nurse, inspired to improve my own practices.
This discussion of hospitals brings to mind the short story “Fidelity” by Wendell Berry (from a collection of the same name). How does the supposed good of “modern medicine” rob a man of his dignity and agency? How do family and neighbors do right by their loved one? When and why is it better to be out of a restless, beeping, impersonal hospital altogether, even in the face of death? A compelling literary perspective on some of the aspects already under consideration here.